


Clinical Case Study: Grady Health, Atlanta, GA.
A Case study, utilizing a novel remote monitoring tablet, directly connected to the Accuryn Monitoring System.
Background:
There are an estimated 300,000 deaths from acute kidney injury (AKI) annually in the U.S.1
A mountain of growing clinical literature has shown that hourly urine output (UO) monitoring may lead to earlier recognition of AKI and better fluid management, thus improving outcomes.2
However, there are multiple obstacles preventing nurses from getting timely readings as well as increased risk to patient care.
THE COVID ICU MONITORING CHALLENGE:
In the COVID-19 ICU setting, it is even more difficult. PPE requirements and patient instability create a chaotic environment for the nurses to record timely urine output for a meaningful fluid balance status. This is because:
- Standard Foley drainage systems have a long history of failing to adequately drain the bladder as well as pose other risks to patients.
- Airlocks and dependent loops trap urine in the catheter, causing inaccurate readings. When nurses “milk” the Foley to move urine into the drainage bag, there is an increased risk of unsterile urine flowing back into the bladder and causing Catheter-Associated Urinary Tract Infection (CAUTI).3
Better Data, Better Outcomes
The Accuryn Monitoring System® overcomes airlocks in Foley catheters and drains the bladder for continuous and automated UO measurements.
By moving urine within a closed loop ventilation circuit, Accuryn removes airlocks to automate urine output. Data is then transmitted to AccuTab, a remote tablet located outside the room.
AccuTab greatly decreases the exposure risk to the staff, decreases the burden of PPE resource utilization and saves precious time. Compared to other urine monitors, Accuryn’s automated drainage provided more accurate and continuous data.4


Results from the Frontlines
Barbara McLean, a clinical nurse specialist in critical care at Grady Health in Atlanta, implemented the Accuryn Monitoring System with AccuTab in their COVID-19 unit.
Implementing the AccuTab outside COVID-19 rooms, Barbara’s team decreased PPE usage and improved their efficiency by having the data they needed outside the room.
Using AccuTab, Barbara noticed a change in urine output that allowed her to intervene.

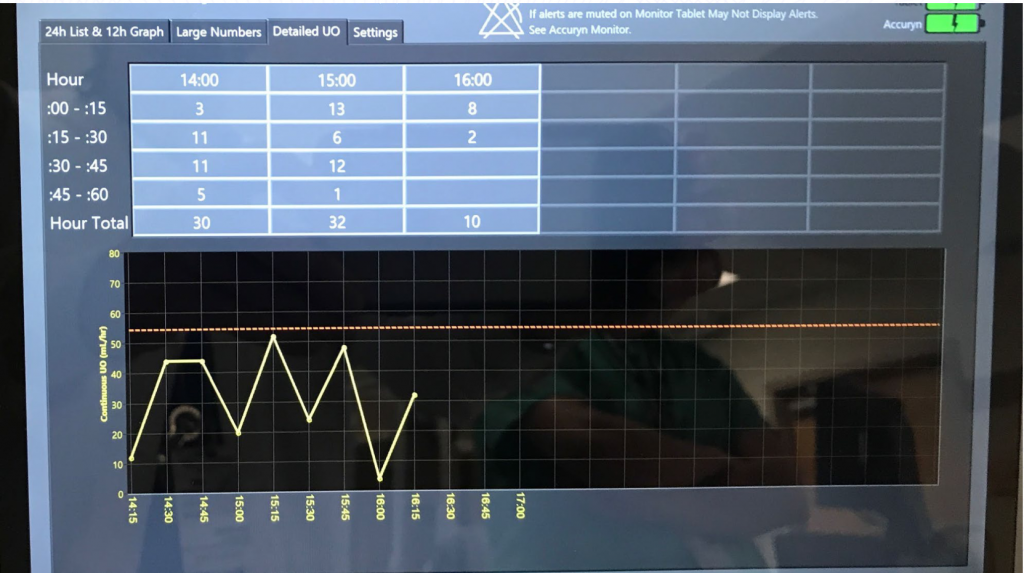
“This dotted line is telling us what the urine output should be to meet the KDIGO guidelines of urine output in milliliters per kilogram per hour” explained Barbara. Anything under this line over time indicates a risk of kidney injury.
At that moment, Barbara notified all attendings, the APC, and bedside nurses.
“I told the team, I’m not suggesting what you’re going to do, but I am suggesting that your
patient does not have appropriate urine output and we must consider doing something”.
Early Data Allows for Early Interventions
The clinical team gave a volume bolus of 500 mL. The result was significant urine output responsiveness, moving the patient safely out of AKI risk.

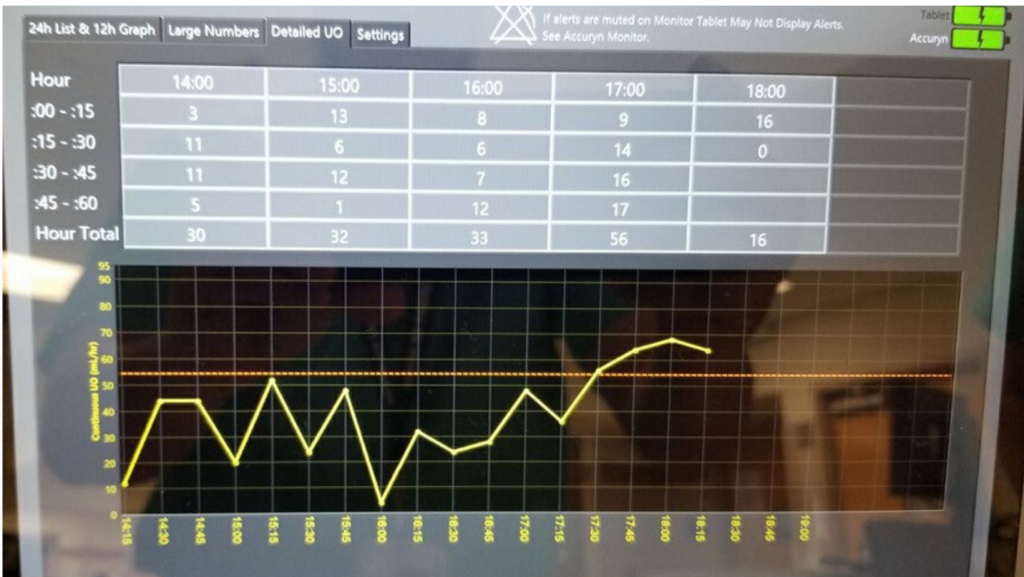
“So that was really important to us because for the care of this COVID patient; we were able to use this fabulous tablet safely outside of the room, to actually tell us what our patient was doing every single hour, what urine output we actually wanted and how our patient was responding to therapy”.
Barbara and her team are happy to report that this patient was successfully discharged from the ICU a short time later. Grady Memorial Hospital continues to utilize the Accuryn system in the COVID ICUs.


References:
1. JLewington AJ, Cerdá J, Mehta RL. Raising Awareness of Acute Kidney Injury: A Global Perspective of a Silent Killer. Kidney international. 2013;84(3):457-467. Available at: https:/ www.ncbi.nlm.nih.gov/pmc/articles/PMC3758780/pdf/nihms463902.pdf Accessed August 24, 2017.
2. Jin K, Murugan R, Sileanu FE, et al. Intensive Monitoring of Urine Output Is Associated With Increased Detection of Acute Kidney Injury and Improved Outcomes. Chest. 2017;152(5):972-979. doi:10.1016/j.chest.2017.05.011
3. Garcia MM, Gulati S, Liepmann D, Stackhouse GB, Greene K, Stoller ML. Traditional Foley drainage systems–do they drain the bladder?. J Urol. 2007;177(1):203-207. doi:10.1016/j.juro.2006.08.101
4. Kramer GC, Luxon E, Wolf J, Inaccuracy of Urine Output Measurements due to Urinary Retention in Catheterized Patients in the Burn ICU. J Burn Care Res . Jan/Feb 2017;38(1):e409-e417. doi: 10.1097