Hills and Valleys is a podcast that uncovers stories from leaders in healthcare, tech, and everything in between. Straight from the heart of Silicon Valley, we give you a look at the good, the bad, and the future, one episode at a time. Brought to you by Potrero Medical.
Listen to the podcast on any of the platforms below, watch the full video interview, or continue reading this blog to see the transcript.
About Dr. Bruce Friedman
Bruce Friedman is the co-director of the JM Still Burn Center and Professor of Anesthesiology & Perioperative Medicine at George Washington University. He graduated from University of Miami School of Medicine in 1983, and has 36 years of experience in the field of medicine.

In addition to practicing medicine, Dr. Friedman has also published extensive research across multiple fields of medicine, including pathology, trauma, burns, and pharmacology.
Dr. Friedman also serves as the Medical Director of Critical Care for Best Doctors Inc, a company that provides technology solutions to employers, providers, and patients.
Earlier this year, Dr. Friedman had a chance to visit the Potrero HQ in Hayward, California. During his visit, he got a tour of the facilities, spoke on sepsis and AKI in the burn unit, and was featured on Potrero’s podcast series, Hills and Valleys. Be sure to keep reading for the full transcript below.
An interview with the co-director of the JM Still Burn Center, Dr. Bruce Friedman
- Interviewer: Omar M. Khateeb, Director of Growth at Potrero Medical
- Interviewee: Dr. Bruce Friedman, co-director of the JM Stills Burn Center in Augusta, Georgia.
Khateeb: Hey everyone. Thanks for joining us today. We are coming to you from our office and headquarters in Silicon Valley here in the media room. Today we have the honor and great fortune to have Dr. Bruce Friedman in the area visiting and we decided to get him into the media room just for a little bit.
So let’s talk a little bit about Dr. Bruce Friedman. He’s coming all the way from Augusta, Georgia. He’s a physician of critical care medicine and the co-director of the JM Still Burn Center over in Georgia, and also a professor in anesthesiology and perioperative medicine.
Considering that we are in March and it’s kidney month, we thought what better way to celebrate it than to talk about acute kidney injury and sort of illuminate some of the problems and also the way technology is being used to solve for that. So, Dr. Freidman, thank you for joining us.
So as we get into it, I want to sort of rattle off a few statistics that were very alarming to me. Being a former med student, I remember learning about the kidney and it is a very difficult organ, but I never knew about these statistics. There is a paper that was written back in 2013 about raising awareness for AKI and it was written by Dr. JP Lewington. And there are some really alarming statistics, you know, 300,000 people die every year alone in the U.S. from AKI, and there’s a chart that shows prostate cancer, breast cancer, heart failure, diabetes, and then AKI is just skyrocketed in terms of the number of deaths it contributes to on average.
It costs a hospital anywhere from three to fourteen thousand dollars to treat, which totals nine billion dollars a year. So it’s a huge huge problem. And the length of stay for a person is about 3.5 days after they get AKI, and 3.5% of the admissions to hospitals get AKI now. One last thing I wanted to show was I decided that, well, that was back in 2013; what about now? I read a paper in 2017, and this is written by doctor GM Shertow, and they found that 8 to 16 percent of hospital admissions actually get AKI, so the problem has not only doubled but tripled in some cases. Why is that?
Friedman: Well, it’s a very good point. One of the things is, and this goes to where hospitals are today, the hospitals today are really acute care centers. Years ago when I first started practicing medicine, we’d admit people that were not very sick, and they’d stay in the hospital and we would get them better and you can’t do that anymore. The people that come to the hospital now have multiple comorbidities. They have very very acute injury. You are getting a higher acuity of patients admitted to the hospital.
What you didn’t mention with AKI is that once a patient gets AKI, their mortality goes up 40%. So in other words, say you’ve got somebody already in the hospital on a mechanical ventilator who is dependent on that ventilator. Then they go into AKI. Their mortality rate, instead of being about 20-30 percent just being on the ventilator, goes up to 70% to 80% during that period that they’re still in AKI. So it’s a devastating effect, and the reason why is because there are two brains, the right kidney and the left kidney. They’re powerful machines. And when that machinery goes bad, lots of things go bad. Toxins appear, you can’t control your electrolytes, your fluids, your acid-base status, all of that changes radically. The only thing you’re left with at that point is putting them on some form of artificial means of support.
Khateeb: And by that you mean something like dialysis, correct?
Friedman: Dialysis, and also what most of us use is the continuous form, which we call continuous renal replacement therapy. And that controls it but it’s a device. It requires a very large central line which carries with it the risk of infection. It doesn’t control everything. Lots of fluid shifting, blood loss, the machine doesn’t work perfectly all the time. There are lots of complications associated with just being on the machine itself.
Khateeb: Interesting. Let’s talk about the admissions then. Eight to sixteen percent is quite high. Sowhen you go into the hospital, how do you get acute kidney injury?
Friedman: Well, most patients that I see in my population is because somewhere along the line there is loss of perfusion to the kidneys. In other words, blood flow and blood pressure gets low, and it doesn’t have to be for a long period of time. It can be for 20 minutes, a few hours, or five hours. It depends on the person, depends on how hardy they are. But once they get exposure to that hypoperfusion for whatever reason, they’re in shock. They have severe congestive heart failure or they have septic shock, burn shock, trauma shock, post-operative shock. The time period they’re exposed to that low blood flow is when they become at risk for acute kidney injury.
Khateeb: And so you know, as it says within the term acute, it’s abrupt and rather quick. How many patients actually know, and not just the patient but even the physicians and nurses, how many of them actually know that they were a victim of an AKI event?
Friedman: Well, you can see it. You start to see a slowdown in the urine output and you begin to see changes in their chemistry. We rely heavily on the simple chemistry such as the BUN and creatinine, and they will go up. They may jump in 24 hours say, from a normal range to maybe one point higher than they were.
Those are your early clues. And they are pretty straightforward clues that you look for that steers you towards okay, well why’s this happening? Was there a period of time that the blood pressure was low? And if there was, there could have been damage to the kidneys. Can we do something to get them better? Are we giving them a medicine that could be affecting their kidneys? Can we improve the forward flow? In other words, from the heart – is the heart not pumping enough. Can we do something about that? Can we do something about the blood pressure? So we start looking for things that we can fix in order to modify the effect on the kidneys. Unfortunately, if exposure to the low-flow was long enough, the kidneys will progressively get worse no matter what you do.
Khateeb: And so you mentioned clues, and I guess that’s the key biomarker is checking creatinine levels. But I believe you need to have a blood draw to check the creatinine?
Friedman: That’s correct.
How Do You Catch AKI Early On?
Khateeb: Let’s imagine a patient who comes out of surgery. They had a little more blood loss than usual in the surgery, so they’re hypovolemic. So maybe there’s damage to the kidney. How common is it that the patient is actually checked and they do a blood draw later on? Is it possible that when those creatinine levels are low or high that they miss the window?
Friedman: Well, they may not you’re absolutely right that they’ll definitely get a test done. If they’ve lost blood they’ll definitely get checked to see if their blood hemoglobin count is low. They may not get a BUN and creatinine check until, say, the next morning. Their urinary output will be monitored very closely. That’s that’s always the case. So you will watch that urinary dynamic, and should give you some idea. Although the standard of care, the current standard of care, is not the best for that.
Khateeb: When you say it’s not the best for urine output measurement, what does that look like at your average hospital?
Friedman: Well, most hospitals are still using a standard Foley catheter with a gravity drainage bag. And, you know, that can give you a false sense of urine function, especially when you’re trying to drain the Foley catheter to get every little bit out of it. You’re going to get wide swings and variability in the urine flow, which may lead you to think that the kidneys are functioning okay, and in reality they aren’t.
Khateeb: And when you say gravity bag, and this is just for those listeners not familiar, it’s just a basic catheter when you walk in and there’s a bag that drains urine. And sometimes there’s a little bit of urine that’s hanging in the catheter and I believe the nurse or a technician comes in and milks that catheter to pull the urine out, correct? So how often is that done usually and how accurate and reliable is it?
Friedman: Our nurses in the ICU setting with the critically ill patients are measuring urine flow every hour. So they’re jotting that down and looking at the collection of the urine every hour.
Khateeb: Got it. And if, let’s say whether it’s an ICU or another department, if it’s very busy and the nurse has different things to do, do we end up seeing a lot of variability in that? Because it sounds like a lot of manual work is being done.
Friedman: Oh, yes. Yes, they will and sometimes it’ll be three or four hours, you know before they look at the total flow. So they may miss a period of time where there was a low flow state and it may be picked up and then it drops back down. So you’re going to miss some of that. You’re going to miss that variability, and that early variability could give you a clue that we’re getting into trouble.
Khateeb: There’s one physician I was speaking with who’s down in Florida, Azra Bihorac, at the University of Florida. Azra mentioned that a lot of patients where AKI is missed are never even aware that they do have AKI. Many of these patients don’t even follow up with a nephrologist after they’re discharged from the hospital. Is that true and have you seen that as well?
Friedman: Well, yeah, I mean that happens. I don’t see that in my practice because I’m totally in patient. I know that it happens because people will go home, for example, from our wound floor population and then they’ll be readmitted for something else having to do with the wound care. And all of the sudden, their renal indices, BUN, and creatinines are up now from the last admission. So they probably did leave with some acute kidney injury that just got progressively worse when they got home.
What’s Preventing AKI Awareness?
Khateeb: As I mentioned before, the kidney is a very very complicated organ. It doesn’t seem like it has as much technological support as, say other organs. So when you have an acute myocardial infarction, there’s stents and a variety of ways to treat that, correct? It doesn’t seem like that’s the case with the kidney. Why is that?
Friedman: Well, there are some things you can do if it’s post bladder, in other words, if it’s obstructed. Then there are urologists who can come in there and stent them and things like that. But those are really not the causes of kidney injury when you block below the bladder, that’s not really AKI. So there are things you can do, but for the kidney itself there really is very little that we can do other than fix the things that affect the kidney.
In other words, like I said before, is there a way we can improve the flow to the kidney by improving the cardiac performance. If the cardiac performance is down, can we can we get that working again by getting better cardiac indices. Or does the kidney just need a little jump start? In other words, has it slowed down because there was a period of hypotension?
Maybe it’s the tubules, and all they need is a little bit of diuretic that to get them back. You know, get them jump-started, and so we give a diuretic. Or, is the patient actually still hypovolemic? Say they’ve gone to surgery: they said they had this much blood loss, but in reality, there’s a lot more. So they need more volume, they need more blood, and that may bring the kidneys back to working level. Having accurate, continuous monitoring of that urinary output then becomes critical to be able to do those interventions, to potentially reduce the incidence of acute renal failure down the line.
Khateeb: And because of a lack of hospitals and technology, at least in the last 10 or 20 years, they haven’t been able to provide that constant monitoring. Do you feel that, for the instance of AKI, that’s one of the reasons why it’s jumped up so much?
Friedman: I think that has definitely contributed to it, yes. Along with, as I said earlier, I think the acuity of patients coming into the hospital is also higher.
Expected Outcomes for Post-AKI Patients
Khateeb: So after a patient gets AKI are they ever really the same? What does that cascade look like? Let’s say a patient gets the classic AKI event. What happens and what does it look like for the next 10-20 years for them?
Friedman: Well many of the patients get better after their inciting event. Whether that’s trauma, burn, a major medical complication of some sort or surgical complication, they get better. They can. Probably 60% get better and their kidney function returns to normal.
But when you have high acuity patients that already have comorbidities – diabetes, peripheral vascular disease, hypertension – who have an element of underlying kidney disease already and then they go into AKI, those patients are less likely to return to normal. They end up on long-term dialysis.
Khateeb: Did they get progressively worse over time?
Friedman: Yes. In fact, older patients with comorbidities who go into an ICU and get AKI, most of them stay in renal failure. Up to 50 to 60 percent of those.
Khateeb: What are some of those comorbidities again?
Friedman: Diabetes, hypertension, peripheral artery disease, those are the most common.
Khateeb: And just for our listeners out there, what’s one of the more common peripheral artery diseases AKI patients have?
Friedman: Any kind of vascular disease that affects the large to medium-sized arteries. Whether it be smoking or whether it be diabetes, long-standing hypertension, or what we call just bad arterial sclerosis. Some people just have a propensity to develop plaque.
Khateeb: That makes sense. A study that was discussed, I believe it was at ASN last year, was that a lot of these patients who were post-AKI or had an AKI event, ten years down the line they were four to six times more likely to have a cardiovascular event. And then some something like four or five times higher to have another, more severe renal issue. Why do you feel that might be the case?
Friedman: Well, I think again the kidney has suffered an injury. If they have any other insult along the way, the kidney will then have less reserve to respond to that. So that makes a lot of sense that they would have problems down the line. We find that the sick ICU patients that go through a devastating illness often have multiple problems after that initial ICU stay.
Khateeb: And unlike the heart, with the kidney we don’t have stents or things like that can go in because the nephrons are pretty small. So we have to just rely on using physiology to its best advantage, which in itself is kind of like a black box, right?
Friedman: Again, there are some things you can do if they have a particular problem in the renal artery in terms of arteriosclerosis or certain autoimmune diseases, but those are very rare. For the most part, trying to recover somebody at AKI is very very difficult.
The Limitations of AKI’s Definition
Khateeb: Something that was really interesting when I spoke with different nephrologists was that they all said a version of what I’m about to share. AKI is a syndrome, but as you just illuminated, there are multiple causes of it; whether it’s drug-induced, cardiac, surgery, all kinds of things.
But it seems that they use AKI as an umbrella term and there isn’t really a delineation of how you treat each of these patients. In other words, it’s kind of a catch-all. Why do you think that is? Why is it that it’s treated as this umbrella term?
Friedman: I think that that’s really the only terminology we have for this. There really isn’t anything else that defines this disease process. So I think that’s where it stands alone.
Khateeb: Do you feel that maybe with better technology or better biomarkers in the understanding of the disease, let’s say diabetic induced AKI versus a surgically induced AKI, that they start being treated differently and approached differently?
Friedman: Well, I think there has to be a difference. You have to distinguish between CKD, which is chronic kidney disease, and acute kidney injury. What we see with the diabetic and the hypertensive and the arterial sclerotic patients, that’s CKD. It’s a progressive worsening of renal function over time. The AKI patient may have these disease states, but may have not manifested CKD yet. But they’re more likely to get into trouble in a serious situation because of their underlying disease states.
AKI in the Burn Unit
Khateeb: In your practice, you deal with a lot of burn patients. So what’s that like with the treatment of burn patients and what are some of the obstacles that you face as a physician with your team in dealing with burn patients and trying to protect them from AKI.
Friedman: The large burns are the most difficult because we have to give them a lot of fluid in the early phases of their burn injury.
They lose a tremendous amount of fluid because of the loss directly from the skin. When you lose the tissue your skin exudes out fluids, volumes of fluid, and those patients are in shock.
They require fluids, but at the same time you have to maintain perfusion or they’ll go into shock. It’s a shock response to the injury. Their vessels dilate down and they get less blood flow to their organs, and one of those is the kidney.
Khateeb: How sensitive are the kidneys of patients who are suffering from burns?
Friedman: Oh, very sensitive.
Khateeb: And is that mainly because of the low amount of volume?
Friedman: That’s right. They’re exposed to low volumes, they are exposed to low blood pressure for periods of time, they are also exposed to some toxins.
For example, people who have gasoline or any hydrocarbon burns, that hydrocarbon can have a direct effect on the kidney so they are toxins. People who have deep burns that involve the muscle or have muscle damage from the burn injury, that muscle breakdown actually causes kidney damage.
Khateeb: So the release of protein and everything puts a lot of strain on the kidney? Interesting. So you have two problems then, one being hypovolemia and then also toxins.
Friedman: Exactly. Yeah, toxins or muscle breakdown damage, what we call Rhabdomyolysis.
Khateeb: And for our listeners, rhabdomyolysis is pretty common, you can get that just from working out really hard.
Friedman: But in these cases it has to do with the depth of the injury. These bigger burns actually get down to muscle. After muscle is damaged, it causes a release of these significant toxins from the muscle tissue that the kidney has to clear, and it can’t. So it’s difficult to have to do things to kind of help the kidney clear that.
Progression of AKI Awareness & Treatment
Khateeb: Historically, lets say 10-20 years ago, what was done to combat this? Comparing that with what’s being done now, if anything has changed.
Friedman: Well, I mean the best thing to do in these situations to help the kidney is to provide the proper amount of volume to continue the best flow towards the kidney.
At the same time, monitor the cardiac function to make sure that you’re getting enough forward flow and perfusion. So it’s really perfusional indices and keeping up with volume losses. Those are the critical pieces.
There’s no magic bullet here. And of course, monitoring that urine output very closely in order to decide what kind of changes you might need to make; whether you need to give more volume, or whether you need to give volume and maybe something to help the heart pump better, those kinds of things. But there’s no magic drug that you can pull off the shelf and reverse the acute kidney injury.
Khateeb: Since we don’t have any great drugs or technologies after the event happens, it’s even more important to monitor and catch these things before they happen.
There’s a story of a girl in Florida whose Apple watch picked up that she might be having a cardiovascular event and she went to the hospital and got treatment. So that was kind of an example of predictive health. Is that how we should start looking at the kidney? Because we don’t have anything that will help a patient post-event, we need to be better about catching it before.
Friedman: The earlier we capture changes in urine output, the more likely we can adjust fluids and inotropic therapy properly. But we really have to stay on top of it and watch those numbers very carefully. I think the earlier we see the changes the more chance we have to reverse the acute kidney injury.
Khateeb: Do you think that by just doing this alone that hospitals, physicians, and nurses, will be able to save those hundreds of thousands of lives I mentioned earlier per year?
Friedman: Well, again, you have to recognize that we’re dealing with a complex group of patients. The idea here’s that if you can take that 40% mortality off the table by stopping or preventing AKI, that’s a big deal. That doesn’t mean the patient won’t die from other reasons because they’re critically ill, but it eliminates one factor.
Khateeb: You really kind of opened my eyes on this.
You mentioned patients being on ventilators earlier and, at least in my knowledge, the only thing I can think of where a patient could go from acute to chronic and still be discharged is with kidney failure. Even then, of course, they’re on dialysis.
The main thing was that in the past, being able to predict and catch those things was difficult. All you could really do if it happened is to help provide renal support to the best of your ability. But with better techniques, technology, and understanding, we can catch these things way earlier on and then start segmenting these patients.
For me, I’m young healthy guy, but I actually only have one functional kidney, right? So it sounds like that’s really the key.
So right now as a physician, when it comes to the management of the kidney, especially in your burn patients, what techniques, technologies do you see coming down the horizon that’s going to help the medical community better addresses AKI and move towards the vision you’re discussing.
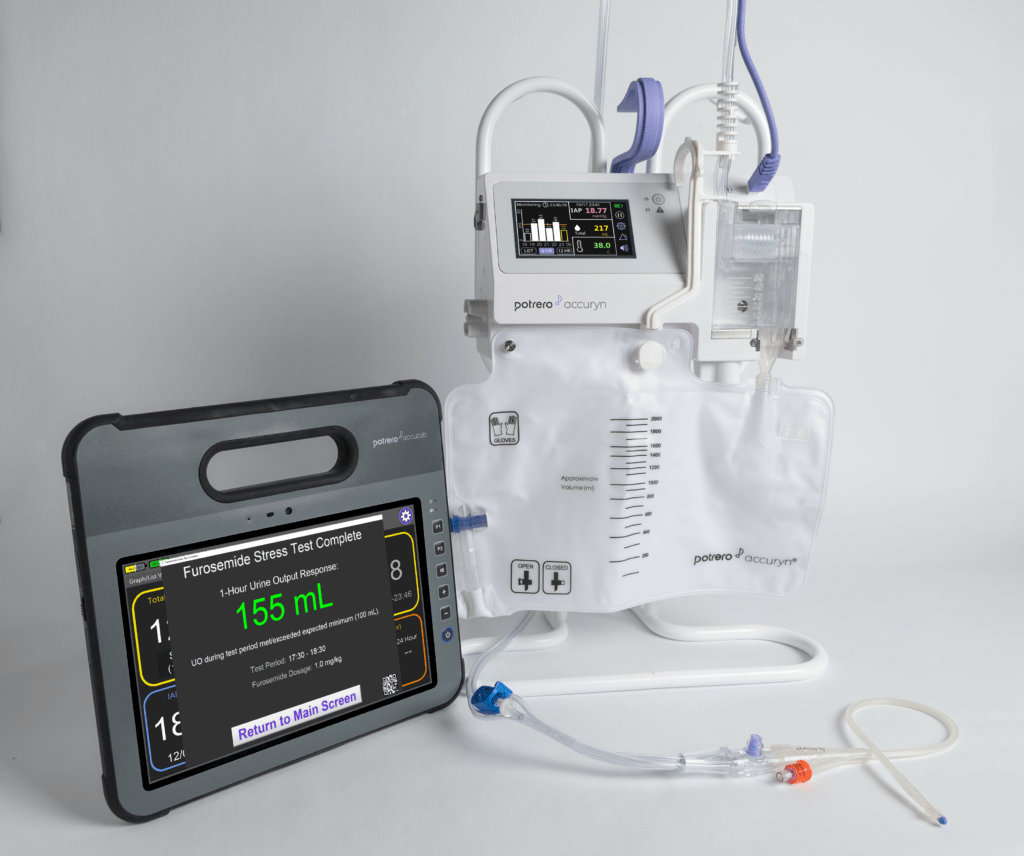
Friedman: Well, the device that we’ve worked with and our did some of the original work with, the initial Accuryn® device. That device has now gone through several changes and has become even more potentially useful in terms of the acute, critically ill, complicated patient.
Having a device like the Accuryn that gives continuous monitoring without damaging the bladder mucosa and can give you urinary output and closely seeing those numbers, that’s something that’s can be very useful in this patient population.
There’s also other artificial intelligence that can definitely be commingled with this device that I think is fantastic. So this kind of intervention put early on into the proper patient population – trauma shock, burn shock, septic shock, post-op surgical shock – these patients would definitely benefit and it could stop them from ever going into AKI.
As we get better with our biomarkers for renal failure, which I think that we will we, may be able to pick that up earlier. Again, looking for intervention.
The one thing that we don’t have though are interventions; in other words, we don’t have that magic bullet. So I think that begs the question that we need something to very very closely monitor the urinary output so that we have an accurate record of that.
This way, we can do as little as we have to do clinically in order to protect the kidneys before they do go into full-blown AKI.
Khateeb: Interesting. And that really does make sense, it kind of illuminates why it’s looked at as an umbrella term because there hasn’t been a way to really monitor those early indicators of AKI.
In the past, a medical team wants to be lucky enough to just stay on top of the urine output and some of these biomarkers just to make sure that they’re maintaining them. There’s not enough time to capture all that data and then start segmenting what urine output and some of these other biomarkers look like.
Friedman: No there’s not, because you’re jumping on this to try to prevent a very acute renal failure issue.
Additional Biomarkers for AKI?
Khateeb: Correct me if I’m wrong, but it sounds like it would be really exciting not just for the medical community, but also for the technology community to get involved.
Because once we start tapping into this kind of data and understanding, then the right therapies and treatments can start coming along to treat each patient differently versus a catch-all.
Right now there’s no data. There’s not enough deep understanding to be able to segment those things and it’s just about keeping them at baseline.
And on topic of biomarkers, I know that the key biomarker for the kidney is creatinine. That and GFR, or glomerular filtration rate. But we are seeing that these are not always as reliable.
Friedman: Correct. That’s right.
Khateeb: We always see a lot of biomarkers discussed when it comes to the kidney at these conferences, but what would you say would be sort of the next thing? Is it limited only to biomarkers?
Friedman: Well, I think that again there are some specific enzymes that have been looked at that are pretty accurate, but not yet totally sensitive and specific.
They have still been shown to be helpful in making the diagnosis of early AKI, but I think even if we get really really good at it, so you can predict it before it happens, what do we do? That’s the question. Right now, we don’t have a whole lot we can do.
One theory is to institute renal replacement therapy early without necessarily doing dialysis but to just to control the volume so you won’t necessarily lose the urine flow that you have.
You can also control some of the toxins that are floating around in the blood and things like that. There’s no true intervention that you can say is going to go directly to the kidney and stop the tubules from getting damaged.
There’s nothing we know of that does that and that’s what we need. If somebody comes up with that, then we’d be in good shape.
Khateeb: Got it. It sounds like before any of that’s done, there has to be an understanding of when and how this happened.
And then physicians can do what they’ve done throughout history, which is okay, now we know when and how this happens. We can now start to decide what we do and do it earlier.
Well fantastic doctor, I really appreciate you spending some time with us. It was very educational. It definitely opened my eyes a lot about why AKI is at the state it is. So before we sign off here, any last thoughts or words of wisdom for us?
Friedman: No, I think that, like I told your folks earlier, I think that you are on the cutting edge here and you are going to save lives, so keep on.
Khateeb: Fantastic, and thank you again for joining us. One last thing is that for those listeners of ours, a lot of them are online and really love to keep up with the guests that we have. Do you have a blog or Twitter or anything online other than email?
Friedman: I actually don’t have a Twitter and I’m not a blogger.
Khateeb: Well that’s just one other good excuse for us to make sure that we have you back again soon, as I’m sure a lot of people have questions. So with that, thank you again.
Friedman: My pleasure.